Claude Gordon Douglas published a method in 1911 that became the gold standard for measuring human metabolism for most of the 20th century. The method is named after the bag he designed to collect exhaled air. It is still occasionally used today as a reference against which modern equipment is validated.
Douglas was born in Leicester in February 1882, the second son of the surgeon Claude Douglas. He was educated at Wellington College and Wyggeston Grammar School, matriculated at New College, Oxford in 1900, and completed his medical degrees in 1907. He spent the rest of his working life at Oxford, attached to St John’s College, where he was a fellow from 1907 until 1949. He was made demonstrator in general metabolism in 1919, reader in 1937, and professor in 1942. He retired as professor in 1949 at the mandatory age and immediately accepted a demonstrator position so he could continue teaching, which he did until 1953.
His scientific career was shaped by his collaboration with John Scott Haldane, whose research group on respiratory physiology Douglas joined in 1908. Haldane was the dominant figure in British respiratory physiology of the period, and Douglas’s career was built within his school. Their work covered ventilation, gas exchange, the regulation of breathing, and the physiology of high altitude.
In 1910 Douglas joined a high-altitude expedition to Tenerife organised by the German physiologist Nathan Zuntz, with Joseph Barcroft from Cambridge and Arnold Durig from Berlin. The following year he was part of the Anglo-American Pikes Peak expedition, where Haldane, Douglas, Yandell Henderson, and Edward Schneider spent several weeks at the summit house in Colorado studying the effects of low barometric pressure on breathing. The results, published in the Philosophical Transactions of the Royal Society in 1913 [1], became foundational reference material for high-altitude physiology. The expedition’s data was the basis for understanding acclimatisation, hypoxic ventilatory response, and the chemistry of how human respiration adjusts to thin air.
The bag
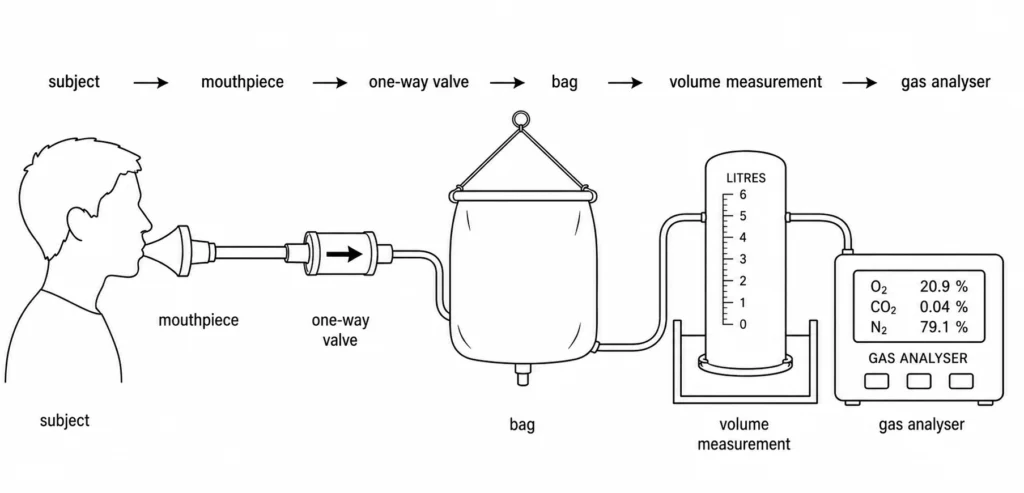
The 1911 paper that gave Douglas his lasting reputation is short — two pages in the Journal of Physiology, titled “A method for determining the total respiratory exchange in man” [2]. It describes a piece of apparatus simple enough to be reproduced in any laboratory: a large canvas bag, lined to limit gas diffusion, with a mouthpiece, a one-way valve, and a stopcock. The subject breathes through the mouthpiece for a measured period — a few minutes, typically — and all exhaled air is collected in the bag. The total volume is then measured, and a sample is drawn off and analysed for oxygen and carbon dioxide content. From those three numbers — volume, O₂ fraction, CO₂ fraction — you can calculate oxygen consumption, carbon dioxide production, and the respiratory exchange ratio, which together describe whole-body metabolism.
The method’s strength was that it was direct. Earlier respirometry had relied on closed-circuit chambers (Lavoisier’s calorimeter, Atwater’s room calorimeter) that were elaborate and expensive, or on indirect calculations from incomplete measurements. The Douglas bag put the apparatus on the subject and let the experiment go where the subject went — onto a treadmill, up a mountain, into the field. It was crude, but it gave full, unambiguous samples of expired gas.
Crude was important for a different reason: the method was robust. The errors are well-characterised and small — gas diffusion through the bag lining, dead-space contamination, valve resistance — and most have known corrections. A careful operator could measure VO₂ to within a few per cent, which is good enough for almost any physiological question.
That combination — directness, robustness, low cost — is why the Douglas bag has outlived the technology that was supposed to replace it. Modern metabolic carts use breath-by-breath gas analysers and electronic flow meters; they are faster, more convenient, and produce continuous data. They are also imperfect, and their calibration has historically been validated against Douglas-bag measurements. A 2017 review in the European Journal of Applied Physiology surveyed a century of error analysis on the technique and concluded that, with appropriate care, it remains valid as a reference standard [3].
What survived
Douglas’s later career was substantial but quieter than his collaboration years. He continued working at Oxford on exercise, respiration, and circulation through the 1920s and 1930s, served on government committees, and trained generations of physiologists. One of his last research students was Roger Bannister, who would run the first sub-four-minute mile a year after Douglas finally retired from teaching. Douglas died in 1963, unmarried, at the Radcliffe Infirmary in Oxford.
The bag itself has had a strange afterlife. The original 1911 design — canvas, rubber, mouthpiece, valve — has been refined but not fundamentally replaced. The same basic apparatus, with better materials, is sold today by laboratory suppliers. Generations of exercise physiology PhDs have done their first metabolic measurements on a Douglas bag, on the principle that you understand the technique by doing it the slow way before trusting the automated version.
The wider methodology Douglas helped to establish — open-circuit respirometry, the systematic measurement of gas exchange to characterise metabolism — is the foundation of every modern claim about VO₂ max, energy expenditure, metabolic rate, and aerobic fitness. A.V. Hill’s 1922-23 work on maximal oxygen uptake, which I wrote about separately, depended on gas-collection methods directly descended from Douglas’s. So does every fitness-tracker estimate of calories burned, every clinical cardiopulmonary exercise test, every elite-athlete VO₂ max number. The instrument has been miniaturised and digitised; the principle hasn’t changed.
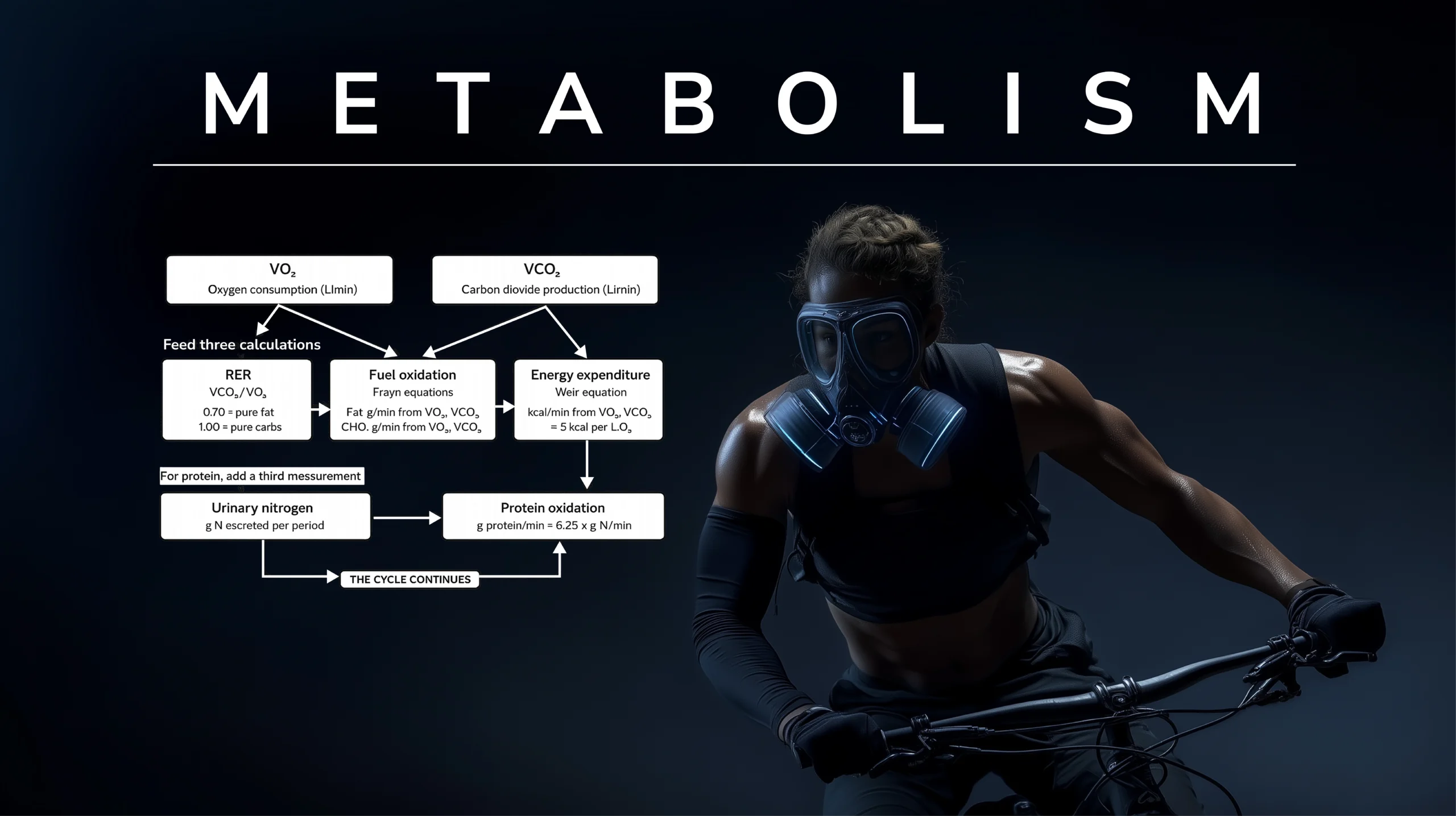
What the same two measurements — V̇O₂ and V̇CO₂ — let you compute is wider than the apparatus suggests. The respiratory exchange ratio (RER, the ratio of the two) is a window onto fuel mix: an RER of about 0.70 indicates pure fat oxidation, an RER of about 1.00 pure carbohydrate, and intermediate values a mixture in proportions that can be read out of standard tables. The Frayn equations (1983) [4] turn V̇O₂ and V̇CO₂ into grams per minute of fat and carbohydrate oxidised. The Weir equation (1949) [5] turns the same two measurements into total energy expenditure in kilocalories per minute — the calorie-burn number that every fitness tracker has been trying to estimate since.
Protein oxidation is the exception that proves the rule. Its RER (≈0.81) sits in the middle of the fat-carb range and can't be separated from gas exchange alone. The full Weir equation includes a urinary-nitrogen term to handle it; acute-exercise calorimetry usually sets that term to zero on the grounds that protein contributes negligibly to fuel use over a short session, and the resulting bias is small. Protein synthesis — tissue being built rather than burned — isn't accessible from gas exchange at all; it requires stable-isotope tracer methods that sit downstream of mass spectrometry rather than Douglas's lineage.
The point is that one piece of 1911 apparatus — a canvas bag, a mouthpiece, a valve — yields, with two analytical refinements published decades apart, a quantitative account of how much fat and carbohydrate an athlete is burning and how many calories they are expending. That is the methodological reach of Douglas's contribution. The bag itself doesn't do the work; the bag plus Frayn plus Weir does the work. But none of the rest of it happens without the bag.
In Afitpilot
Afitpilot sits an entire methodological generation downstream of the Douglas bag — and currently captures none of it. The platform handles strength load through an estimated 1RM derived from per-set reps, weight, and optional RIR, and handles overall training stress through Foster's sRPE × duration. It has no gas-exchange measurement, no VO₂ estimate, no heart-rate capture, no HRV, no wearable integration, and no representation of energy expenditure in kilocalories or kilojoules. Endurance work enters the platform as session duration and perceived effort, not as aerobic capacity or oxygen kinetics.
-
Session RPEBorg CR10, multiplied by duration (Foster 2001) → arbitrary units of training loadFoster 2001
-
Reps in reservePer-set, 0–4. Feeds the estimated 1RM (Epley) calculation per exercise.Zourdos 2016
-
Daily readinessFive-item Hooper index: sleep, soreness, fatigue, mood, stress, 1–7 each.Hooper 1995
-
Weekly AU + acute/chronic trendEWMA over 7- and 28-day windows. Descriptive only — no injury-prediction signal.Impellizzeri 2020
-
VO₂ maxNo direct measurement, no estimate, no wearable input.Douglas 1911
-
Calories / energy expenditureNo METs, no kJ, no kcal field anywhere in the schema.—
-
Heart rate / HRVNo resting HR, no zones, no variability.—
-
Wearable integrationsZero. No Apple Health, Garmin, Strava, Whoop, Oura, Polar.—
The omission is partly principled and partly just where the roadmap currently sits. The principled part: the input layer the platform has built — sRPE, RIR, daily readiness — is everything an athlete can self-report without instrumentation, which keeps the cost of using the system to zero hardware. Instrumented inputs bring their own measurement problems (consumer-grade HR variance, wearable-to-wearable disagreement on VO₂ estimates, the noisy ground truth of any device that isn't a metabolic cart) and integration problems (vendor APIs, sync reliability, the data-portability story for athletes who change devices). Building the wearable layer well is not a small piece of work, and shipping it badly would import noise into a stack that's currently built around inputs the athlete controls.
The unprincipled part: the entire half of physiology Douglas's lineage opened up — oxygen kinetics, energy expenditure, aerobic ceiling, autonomic recovery — lives outside the platform's current model, and it shouldn't forever. A wearable integration that surfaced heart rate, heart-rate variability, and an estimated VO₂ max would let the platform represent endurance training as something other than "minutes spent at perceived effort N." That work is on the roadmap; it is not built today.
I wrote separately about A.V. Hill, whose work on maximum oxygen uptake built directly on the gas-collection methods Douglas established.
References
References
[1] Douglas, C.G., Haldane, J.S., Henderson, Y., & Schneider, E.C. (1913). Physiological observations made on Pike's Peak, Colorado, with special reference to adaptation to low barometric pressures. Philosophical Transactions of the Royal Society B, 203, 185–318.
[2] Douglas, C.G. (1911). A method for determining the total respiratory exchange in man. Journal of Physiology, 42(Suppl), 17–18.
[3] Shephard, R.J. (2017). Open-circuit respirometry: a brief historical review of the use of Douglas bags and chemical analyzers. European Journal of Applied Physiology, 117(3), 381–387.
[4] Frayn, K.N. (1983). Calculation of substrate oxidation rates in vivo from gaseous exchange. Journal of Applied Physiology, 55(2), 628–634.
[5] Weir, J.B. de V. (1949). New methods for calculating metabolic rate with special reference to protein metabolism. Journal of Physiology, 109(1-2), 1–9.
Leave a Reply
You must be logged in to post a comment.